Name - Physales Micrantha Link - 3 Age - 40 Sex - F dt. 06.04.18









What follows is an update of what transpired after that when the patient finally arrived for a necessary intervention to our hospital (17/04/2018).

An MRI of the ovaries was done on the same day and the patient taken up for surgery the same day also in view of her severe abdominal pain that was initially thought to be an ovarian torsion and a surgery was done.







Postoperatively she developed fever, hypotension, tachypnoea and crepitations were noted in the chest. Chest X-ray was suggestive of bronchopneumonia. The pictures are as follows:
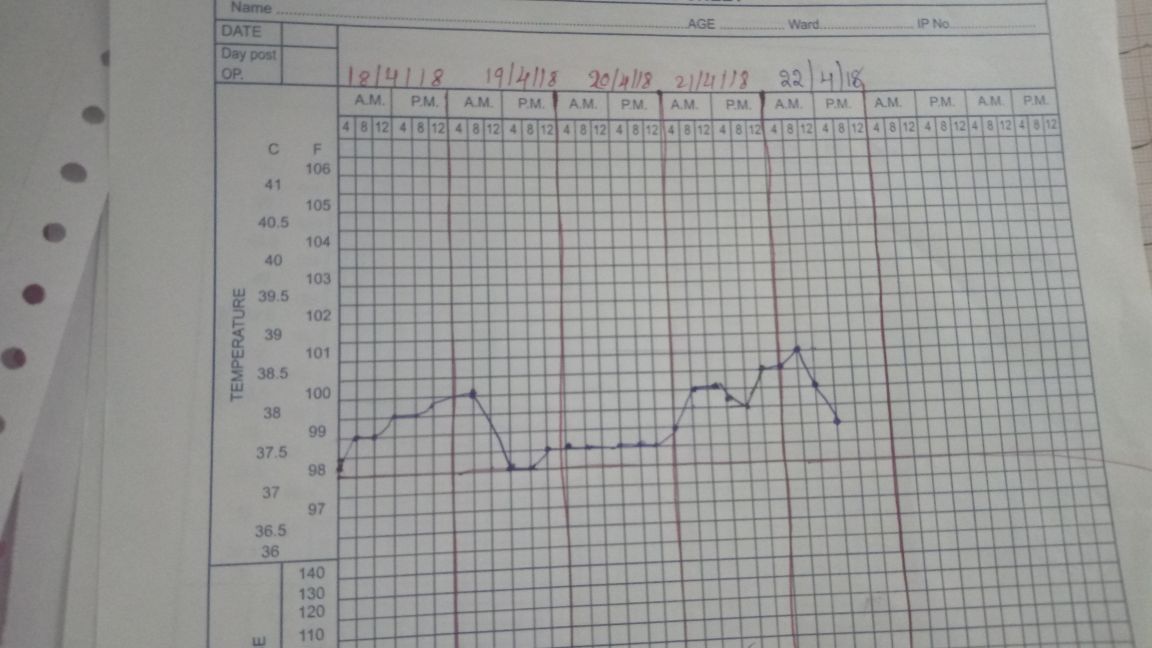

Appeared to have disseminated pulmonary involvement. In view of her severe abdominal pain radiating to the back, the chances of ovarian malignancy are high so one of the possibilities is disseminated malignancy over disseminated tuberculosis. The ovarian tissue removed during OT last week should be reported by tomorrow. We have started a fentanyl patch for her persistent pain. Her fever continues relentlessly although sepsis hypotension has reduced and currently, she is no longer on inotropes with noradrenaline tapered off the day before yesterday (22/042018).

The Update on the 26th April 2018:
There is an interesting twist to the case.We got to see the microscopy of her removed ovary today.




There is an interesting twist to the case.We got to see the microscopy of her removed ovary today.



The thecoma component of the ovarian tumor

fibroma component of the Ovarian Carcinoma.


Fibro thecoma of the Ovarian Component
Rakesh Biswas: How do we make sense of her fibrothecoma of the ovary, her pulmonary nodules and pleural effusion as in her CT and her severe abdominal pain? An MBBS short note often asked in the OBG exams by the name of Meigs syndrome suddenly rang a bell.
Here's a similar thecoma with abdominal pain due to sclerosing peritonitis.
https://journals.lww.com/intjgynpathology/Abstract/2014/01000/Fatal_Case_of_Luteinized_Thecoma_With_Sclerosing.5.aspx
Another report of an "ovarian
fibrothecoma tumour with metastatic disease in the small intestine and peritoneum," in the PDF below.
Similar in the sense that,
"their vascular pedicle, limited contrast enhancement, and pain described by the patient suggested possible torsion. They, therefore, performed an emergency exploratory laparotomy."
Here's a similar thecoma with abdominal pain due to sclerosing peritonitis.
https://journals.lww.com/intjgynpathology/Abstract/2014/01000/Fatal_Case_of_Luteinized_Thecoma_With_Sclerosing.5.aspx
Another report of an "ovarian
fibrothecoma tumour with metastatic disease in the small intestine and peritoneum," in the PDF below.
Similar in the sense that,
"their vascular pedicle, limited contrast enhancement, and pain described by the patient suggested possible torsion. They, therefore, performed an emergency exploratory laparotomy."
Fatal Case of Bilateral Luteinized Thecoma with Sclerosing Peritonitis in a 33-Year-Old Woman
(The link to the case report is below)
https://drive.google.com/file/d/1rme-ZVhUcUJ56XaVd_vsL_LH-_GZhC6Q/view?usp=sharing
Malignant fibrothecomatous tumour of the ovary: Diagnostic value of anti-inhibin immunostaining (the link to the paper is below)
https://drive.google.com/file/d/1ueJRIyfA1VNyb80-Uk8lrtF6XtXrujb5/view?usp=sharing
28/04/2018: Another twist today to the patient previously:
Can't justify our missing the glaring findings in her neck during the day of admission just because we were overtly distracted by her severe abdominal pain mimicking ovarian torsion and I admit it felt really embarrassing today to have the delayed realization of having missed such significant lymphadenopathy in her neck.
We quickly tried to rectify that by obtaining an FNAC of the lymph nodes followed by an excision biopsy today itself.
The FNAC image of the patient's lymph nodes:

FNAC Report:

Lymph node biopsy sample currently preserved in ICU frig:

The other close differential for our patient after today's discoveries
"Because of the diverse manifestations of Castleman disease and its ability to affect any body region, Castleman disease is a great mimic of both benign and malignant findings in the neck, chest, abdomen, and pelvis. Castleman disease includes a spectrum of pathologic variants, including the classic hyaline vascular Castleman disease and the less common plasma cell Castleman disease." Here too ours appears to fit into the less common variety of this uncommon disease.
https://pubs.rsna.org/doi/full/10.1148/rg.316115502
Last update:
On a night duty day in ICU after explaining the nursing staff about the investigations to be sent the coming morning for the patients in the ICU, and the necessary work to be completed before the dawn arrives, I had left to my duty room to catch a nap as I had a long day coming ahead. It was almost 1 hour later when I got a call from the ICU asking me to attend a patient as her blood pressure and pulse were not recordable.
Still in half sleep struggling to open my eyes and getting my senses into place I tried to recall what would have happened to her as I had seen her 1 hour back wincing out loud in pain. I rushed to the ICU where I see 2 persons from the nursing staff trying to wake her up, shouting out loud, while the other nursing person had understood the scenario and had arranged the CPR and the intubation tray with the necessary equipment.
I could sense the shiver in my spine and my heart shouting out loud, "is this the end?" While I was going ahead with the CPR with the nursing persons in turns. Had called my team members to ICU urgently who were on duty that particular gloomy night.
My team had arrived half exhausted half asleep after a long day, they assissted us in the CPR where all of us took turns in reviving her. I could see the questions in every one's eyes probably asking each other with their eyes whether is this it what we had imagined.
After trying to revive her for 40 min we had taken the call to declare her dead. The nursing staff had handed over me a bunch of papers to be filled, the formalities to be completed, the calls to be made to intimate the administration about the death, the search for the closed ones of the deceased.
While I was filling the papers and completing the formalities I asked the staff there to call up the administrator on duty as I knew he would know what exactly had to be done after the formalities. The closed ones rushed in with so much fear in their eyes as they had been woken up from their sleep stating the urgent need of them in the ICU. Still completing the papers I see the son who rushed to his mother and shaking her up vigorously shouting out to wake her up, with tears rolling down his eyes he still was trying to wake her up, his wife had left to intimate their relatives 2000kms away from this hospital about the unfortunate dawn which they had expected to occur but probably some months later.
My eyes filled up with tears on seeing a son a loved one trying to wake his mother up from a deep sleep from which no one has come back. He had booked his tickets to go to their home town with the patient along 4 days later. Nevertheless he hadn't wondered in his frightest thought about the end being so near. I sat there with a sad heart recalling the previous night when I had seen her and imagined in the fraction of minute as to how painful it was for her, she couldn't sleep nor could she sit. She couldn't breathe but nor did she want a oxygen mask over her face. We had inserted a ryles tube suspecting a intestinal obstruction and she begged us to remove it that night. She had begged her son to remove it but he didn't want to do so and neither could he explain his mother that removing it was not a wise decision. All these ran through my mind when I hear my phone ring. I got a call from Casualty asking for help for a case.
On my way to casualty I once again got reminded of how imprecise medicine was. We had a lady suffering with a disease in the end stage and all we had to do was to make her last days comfortable, which we were unsuccessful at. Because in the recent few days we had done a biopsy of her lymph node, loaded her with iv contrast for the radiology imaging, tried securing cannulas so many times in her edematous limbs. She had definitely gone through much pain in the last few days. The imprecision of the medicine again stands up, as we knew what she was suffering from, but could we help her? Could we provide the peace and comfort in her last few days on this Earth? Could we assure her with precision that you will be living for these many months or years.. we could do nothing. Nothing which would have helped her or which would have comfort her.
Medicine has advanced so ahead in the past few years but still we could do nothing to help her, to soothen her pain. She had come all the way from her home town tavelling for 2 days to help get rid of her pain which she had been having since the 2 months. Has medicine given her the intimation of the precise time which she was left with?
Probably this is the way it works, being imprecise, striving for precision, because medicine cannot intimate a person regarding the precise time one has been left with. Would precision in such events of life and death help us in any way or is it better to be imprecise in few areas of life is left for us to decide.
A new dawn for everyone but sadly for a family it had been quiet unfortunate.
This comment has been removed by the author.
ReplyDeleteHistory after translation from Bangla:
ReplyDelete1. I had no problem during childhood.
2. My period was started at the age of 13 years and was everything alright then.
3. I was married at 17 years of age and got birth to a child with normal delivery after a year.
4. In 1996, after delivery (not sure if it is second as the word was not clear), I was being ligated and since then every time during my periods I started getting pain which was never before present.
5. From last 1 and half months, I am feeling severe pain which is intolerable. It is associated with a daylong fever which is higher at night. I also feel shortness of breath.
6. I have indigestion, anorexic, insomnia, constipation, yellowish urine with reduced feeling of thirsty. I get shocked (could not translate into a more medicalized term) if someone try call me suddenly.
Presentation
ReplyDeletehttps://bmjcaselogvivek.blogspot.com/2018/10/presentation-on-fibrothecoma.html